As a beginner in hospital clinical medicine, my initial struggle, besides perpetually low caffeine levels, was trying to get a handle on the seemingly vast comprehensiveness of the management plan needed to cover all aspects of care from admission to discharge in a timely manner. It often got overwhelming and made me feel nervous, unorganized & unsatisfied. I came up with a mental framework to help tame that comprehensiveness to more manageable, analytical chunks of thought processing – no matter what the clinical issue is.
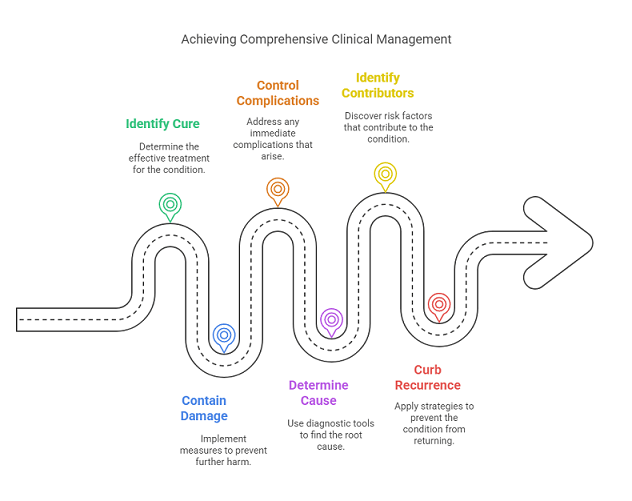
Here’s the 6-Cs Clinical framework which might benefit other beginners:
Cure : What is the cure for the condition ?
Contain further Damage: If no cure or awaiting cure, what can be done to contain further damage?
Complications control: prevent or treat any direct complications of the condition
Cause determination: What Labs/Imaging/Procedures are needed to identify a direct cause ?
Contributors : What Labs/Imaging/Procedures can identify contributors (or risk factors) to treat?
Curb recurrence risk: What Interventions can you do to curb or cut risk of this re-happening? (secondary prevention)
A beautiful example for the framework is ischemic stroke management
Cure: Eligible for tPA or endovascular intervention? If not then focus on controlling the damage
Contain damage: avoid fevers, hyperglycemia, and uncontrolled BP to preserve stroke penumbra & improve recovery
Complications to prevent/treat? : Aspiration (keep NPO, have speech pathology see), pressure sores, fall risk (consult PT/OT), Depression, DVT
Cause analysis: EKG, Telemetry, ECHO, Carotid Duplex, Viral panel to screen for AFib, Cardiac clots, PFO, Carotid stenosis, COVID, etc.
Contributors: Screen for risk factors w/ A1c, Lipid Panel, HTN history, sleep apnea, etc.
Curb recurrence risk: Secondary prevention with ASA/Plavix/Anticoagulation along with BP/DM/Cholesterol control
Let’s take something surgical such as a Fracture:
Cure = surgical fixation – consult orthopedics, do a quick pre-op eval
Control damage: immobilize the fracture area with a splint while awaiting surgery since movement & weight bearing can worsen it
Complications to prevent/treat: Blood loss anemia? Pain & spasm? compartment syndrome?
Cause: Trauma? Fall? Syncope ruled out? (Fall: Vit D def. , Neuropathy, Alcoholism, orthostatic )
Contributors: Osteoporosis? Vit D. deficiency ? / Neuropathy causing falls? – B12/Folate/Alcoholism.
Curb recurrence risk: Rehab, Address Osteoporosis (Give Bisphosphonates), address malnutrition
Don’t miss these fun posts! Subscribe via email 📩 | |